Psychotherapy Articles
Psychotherapy Articles

Parallel Process in Multicultural Supervision
One of my best friends is a skilled storyteller. During our internship year, she would regale the staff of the counseling center with tales of suspicious occurrences surrounding Area 51, the “secret” government location where UFOs are purportedly stored and studied. She would wax on about mysterious sightings and disappearances with oratory inflections akin to a female Rod Serling. She always ended her yarn with the animated phrase, “Coincidence? I think not!”
How is this relevant to parallel process and multicultural supervision? I invite you to consider the back-to-back articles published in Psychotherapy Volume 49(3), in which Tracey, Bludworth, and Glidden-Tracey (2012a) provide evidence for parallel process in supervision and Watkins (2012) questions the veracity of the claim by saying, “What might be construed as parallel process, might be real process that parallels” (p. 345). Is what “has become the best-known phenomenon in supervision: perhaps even the signature phenomenon,” (Bernard & Goodyear, 2014, p. 65) simply a coincidence?
Tracey et al. (2012a) analyzed patterns of dominance and affiliation between pairs of clients and trainees and trainees and supervisors, finding that “[supervisors and trainees] altered their behavior from their own general patterns in line with what would be predicted by the theory of parallel process” (p. 339). Client and trainee dyads were more similar on dominance and affiliation in the beginning of therapy than trainee and supervisor dyads, then became increasingly dissimilar mid-treatment, during which time the most successful trainee-supervisor dyads became more similar. Toward the end of therapy, client-trainee similarity ratings increased again. The results supported the contention that “The trainee brings the ‘less adaptive’ behavior of the client into supervision, and the supervisor and the trainee enact a minor version of the same interaction…then the supervisor alters her/his behavior away from these client-defined patterns, theoretically with the intention to promote alternatives for the therapist to employ in the session” (p. 340). Positive client outcome was associated with a pattern in which the trainee’s behavior resembled the supervisor’s mid-treatment.
For Watkins, the crux of the issue centers on whether unconscious processes are at play. Is the supervisee unconsciously enacting the client’s process in supervision? Was there sufficient evidence to claim that client-therapist dynamics get played out in supervision and vice versa? In their response, Tracey, Bludworth, and Glidden-Tracey (2012b) asserted that they “found strong support for the presence and value of an interpersonal conception of parallel process in supervision” (p. 348) that might reflect but not preclude an unconscious element.
The purpose of this article is twofold: a) to step outside of an either/or mentality about parallel process and adopt a stance of both/and (Hardy, 1995), given that parallel process may be both an unconscious replication of intrapsychic dynamics and an interpersonal one; and b) to examine how parallel process in multicultural supervision may be both a resource and a liability. Unnoticed and unexamined unconscious processes and interpersonal behaviors may be transmitted in either direction across the therapeutic triad (Doehrman, 1976) and may have positive or negative effects. It is the trainee who is operating in the middle of these dynamics (Frølund & Nielsen, 2009) and is both reflecting and mirroring the inter- and intra- personal dynamics of the client and supervisor. By taking a both/and stance, parallel process may be recognized as both a vehicle for the transmission of bias and a conduit for identifying and reducing biased practices and promoting or enhancing culturally responsive psychotherapy (Inman & DeBoer Kreider, 2013; Ladany, Inman, Constantine, & Hofheinz, 1997).
One way bias is communicated is through microaggressions (Sue et al., 2007). “Microaggressions are the everyday verbal, nonverbal, and environmental slights, snubs, or insults, whether intentional or unintentional, that communicate hostile, derogatory, or negative messages to target persons based solely upon their marginalized group membership” (Sue, 2010, p. 3), and are associated with a range of negative attitudes towards singular (Sue, 2010) and intersecting cultural identities (Lewis & Neville, 2015). Microaggressions are often delivered by well-meaning individuals who are oblivious to the impact of their behavior. According to Sue (2010), microinsults (rude, demeaning insensitive comments or actions) and microinvalidations (diminishing behaviors or statements that nullify or redefine the target person’s own phenomenology) are often unconscious (p. 8), whereas microassaults (explicit words or actions that denigrate and intend harm) are often conscious and intentional.
Microaggressions create “psychological dilemmas” (Sue, 2010, p. 11) among and between people (Sue et al., 2007; Zetzer, 2015), including clients and trainees and trainees and supervisors (Bartoli & Pyati, 2009; Constantine & Sue, 2007; Hernández, Carranza, & Almeida, 2010; Murphy-Shigematsu, 2010). Microaggressions are unavoidable. Even the most committed psychologists and trainees are going to bumble into them. Each of us holds both the propensity to emit and the potential to reduce the likelihood of enacting microaggressions.
Microaggressions and parallel process are complementary constructs, and supervisor self-knowledge is the bridge between them. Self-knowledge includes awareness of the historical and cultural context for the expression of intersecting identities and “awareness of the effects of one’s behavior on others, and changing behaviors that no longer serve healthy growth or relationships” (Butler-Byrd, 2010, p. 12). For example,[2] I identify as a White, 50-something, LGBT ally, who is committed to social justice and a feminist multicultural approach to psychotherapy and supervision. While supervising a case transfer between trainees, I intentionally paired a sexual minority client with a sexual minority trainee because I thought that the client would benefit from working with a positively identified sexual minority therapist. Without thinking twice, I encouraged the transferring therapist to describe the benefits of the arrangement with the client. Shortly thereafter, the client left therapy.
What happened? I trust that you can generate many hypotheses, but it may be helpful to look at this from the standpoint of microaggressions and parallel process gone awry. The transferring trainee brought the client’s internalized oppression related to their[3] sexual orientation identity (Worthington, Savoy, Dillon, & Vernaglia, 2002) into supervision and expressed the hope that the client would become more self-affirming. The client was a sweetheart and the first trainee and I liked the client tremendously. Here was someone who deserved the kind of love and care that flows to people who feel worthy. The trainee and I felt a “pull” (Hill, 2014) to make life better. Now, here is the key: Our response was a “microinvalidation,” a set of actions that denied the reality of the client’s experience as a sexual minority who was raised in both a loving and homonegative family and is living in a heterosexist culture. The incoming clinician saw this instantly and confronted me about process and the outcome. The new trainee’s experience mirrored that of the client. That experience said, “We know what you need,” and “Here’s what you should do.”
Defining someone else’s contribution is a hallmark of privilege (Zetzer, 2011), and it is connected to structural/institutional forms of oppression (Reynolds, 1997). Outing the new clinician and prescribing a certain type of relationship was a significant error with a real consequence. Uncontaminated attunement to parallel process and vigilance regarding microaggressions might have led to a more positive outcome. I feel fortunate that I was able to repair the relationships with the trainees. I am especially indebted to the incoming trainee who spoke candidly to me. We have worked closely together since then and while this represents a “tear and repair” (Beutler & Harwood, 2000) of the supervisory relationship, there was no repair in the relationship with the client. They left.
This is an example of parallel process as a liability. One way to guard against repeating this mistake and to move toward making parallel process an asset is to apply a model of multicultural supervision that relies on both self-knowledge and an external framework. Inman and DeBoer Kreider (2013) defined multicultural supervision and counseling competence as “the development of an understanding of the contextual and systemic issues on each member of the client-counselor-supervisor triad, as well as the process and outcome of counseling and supervision” (p. 346). They offered two approaches to supervision that would have been useful in my first case example.
The Critical Events Model (CEM; Ladany, Friedlander, & Nelson, 2005) is a systematic approach to multicultural supervision that can be used to map out complex intra- and inter- personal interactions into events that have a beginning, middle, and end. The event begins with a “marker” that is observed by the supervisor or trainee. Markers are discontinuities in the therapeutic or supervisory process. According to Ladany et al. (2005), once a marker is identified the supervisor moves into the “task environment” and applies interventions to supervision with the intention of cultivating culturally competent responses on the part of the trainee. If successful, the task environment leads to the resolution of the critical event. In this case example, noticing critical markers would have resulted in greater attunement with the client’s experience of internalized oppression or greater awareness of my unabashed hopes for client change. Such awareness would have led me to offer a different task environment.
As a supervisor, I would also have benefited from using Ancis and Ladany’s Heuristic Model of Nonoppressive Interpersonal Development (HMNID; 2010) to draw attention to how a trainee’s and supervisor’s membership in a “socially privileged group” (SPG) and/or “socially oppressed group” (SOG) may influence psychotherapy and supervision. The first trainee and I were responding from our sociopolitical locations (Watts-Jones, 2010) as members of an SPG. The client and second trainee viewed the case transfer process as members of an SOG. All four of us have multiple memberships in SOGs and SPGs. However, the locations related to sexual minority/majority status are the most salient for understanding the outcome of this case.
Sociopolitical locations related to race/ethnicity, gender, and class were the most salient features of a second case example, in which parallel process was used to foster a more positive outcome (Zetzer & Reese, 2014). I supervised an Asian American male trainee working with a 30-something Asian American female client who sought therapy for depression caused by the sudden termination of an engagement with a European American man who was ten years older. He borrowed a large amount of money from her, cheated on her, and then ended the relationship. He was exploitive, coercive, and violent while they were together. However, she missed him terribly and wanted him back.
The trainee administered weekly measures of outcome and the therapeutic alliance using the Partners for Change Outcome Management System (PCOMS; Duncan, 2012). At session three, the client’s sense of wellbeing, as measured by the Outcome Rating Scale (ORS) indicated reliable deterioration. She told the trainee that she was looking for ways to reunite with her ex- to get her money back. At session four, the total ORS score continued to decline and the quality of the therapeutic alliance, as measured by the Session Rating Scale (SRS), showed deterioration. The client wanted direction. The therapist asked me for direction. I focused my concern on the client’s safety and directed the trainee to work with her to form a plan in case she met with her ex-partner and he became abusive. I insisted that they work together to build the plan even after he said, “She won’t like it.”
Session five went poorly and the Total SRS score did not change. The client said she was confused. The trainee came into supervision feeling confused. Then, I felt confused. How could a call for a safety plan, clearly a demonstration of caring, elicit so much confusion? Though this trainee was highly skilled at cultivating therapeutic relationships, the low SRS score (31 out of 40) suggested that the alliance was weak (36 and below is cause for concern; Miller & Duncan, 2004; see Figure 1.) Hence, there were two markers: a) the confusion and b) the low SRS scores.What is a feminist multicultural supervisor to do? Look for the intra- and inter- personal dynamics of power and privilege in the triadic relationship (Enns, 1997). I hypothesized that neither the client nor the therapist felt safe enough to challenge authority. I wondered how race, gender, and class differences were contributing to the interpersonal dynamics. Perhaps the client’s assertions of autonomy and capability were being expressed in a culturally consonant manner as “confusion” and carried by the therapist into supervision. After recognizing the parallel process, I immediately moved to a one-down position with the trainee and said, “Oh my! I have asked you to take a position of authority with a client who has been disempowered in relationships all her life. I am sorry. What do you think should happen next?” The trainee suggested that he ask the client the same question, and voilà! The next session the total SRS score increased. Despite continued fluctuations, by session 10 the ORS revealed reliable, but not clinically significant, change (from a low of 11.8 to a high of 21.8) and the SRS score was 35.9.
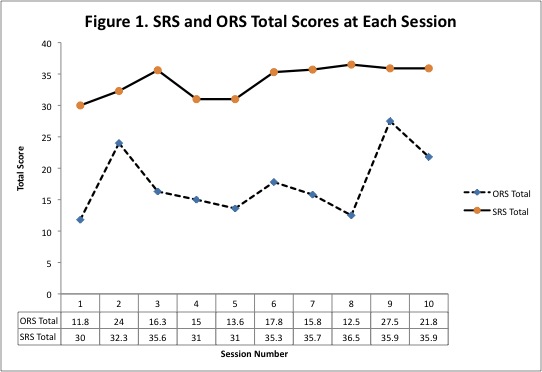
Figure 1. Total Outcome Rating Scale Score (ORS) and Total Session Rating Scale Score (SRS) Per Session. Range is 0-40. Higher scores are better. Reliable change index for ORS is 6. Total ORS scores below 25 suggest client’s sense of “how well” they are doing is similar to an outpatient population. SRS scores above 36 are desired.
It is my interpretation that the trainee brought the “less adaptive” behavior of the client into supervision by reporting confusion (Tracey et al., 2012a, p. 340). Fortunately, after much feminist soul-searching and some obvious empiricism, I was able to step back and take a more reflective, collaborative, honoring, and empowering stance with the trainee, who offered that same shift to the client, who in turn showed improved sense of well-being and greater satisfaction with therapy.
Adopting a both/and stance towards parallel process allowed me to use critical event markers to reflect on practice (Schön, 1983) and then hypothesize about invisible internal states (e.g., internalized oppression, unconscious privilege) as they were elicited and expressed in the visible interpersonal interactions across the therapeutic triad. By witnessing the ways in which trainee behavior paralleled that of the client, I was able to observe and then select interventions in the “task environment” that supported culturally responsive interventions on the part of the therapist—and that led to improvement.
Coincidence? I think not!
[1] Author’s Note: Portions of this article were presented at the Society for Counseling Psychology Conference, Atlanta, Georgia, March, 2014.
[2] Identities of trainees and clients have been de-identified and disguised throughout this article.
[3] I am using the plural pronoun to both mask the gender of the client and to remind the reader of the fluidity of gender identity and the binary hegemony that we see in the English language.
Cite This Article
Zetzer, H. (2015). Parallel process in multicultural supervision. Psychotherapy Bulletin, 50(2), 19-23.
References
Ancis, J. R., & Ladany, N. (2010). A multicultural framework for counselor supervision. In N. Ladany & L. J. Bradley (Eds.), Counselor supervision: Principles, process, and practice (4th ed., pp. 63-90). New York, NY: Brunner-Routledge.
Bartoli, E., & Pyati, A. (2009). Addressing clients’ racism and racial prejudice in individual psychotherapy: Therapeutic considerations. Psychotherapy: Theory, Research, Practice, Training, 46(2), 145-157. doi: 10.1037/a0016023
Beutler, L. E., & Harwood, T. M. (2000). Prescriptive psychotherapy: A practical guide to systematic treatment selection. New York, NY: Oxford University Press.
Bernard, J. M., & Goodyear, R. K. (2014). Fundamentals of clinical supervision (5th ed.). Saddle River, NJ: The Merrill Counseling Series.
Butler-Byrd, N. M. (2010). An African-American supervisor’s reflections on multicultural supervision. Training and Education in Professional Psychology, 4(1), 11-15. doi: 10.1037/a0018351
Constantine, M. G., & Sue, D. W. (2007). Perceptions of racial microaggressions among Black supervisees in cross-racial dyads. Journal of Counseling Psychology, 54(2), 142-153. doi: 10.1037/0022-0167.54.2.142
Doehrman, M. (1976). Parallel process in supervision and psychotherapy. Bulletin of the Menninger Clinic, 40(1), 3-104.
Duncan, B. L. (2012). The partners for change outcome management systems (PCOMS): The heart and soul of change. Canadian Psychology, 53(2), 93-104. doi: 10.1037/a0027762.
Enns, C. Z. (1997). Feminist theories and feminist psychotherapies: Origins, themes, and
variations. Binghamton, NY: Harrington Park Press/Haworth Press.
Frølund, L. & Nielsen, J. (2009). The reflective meta-dialogue in psychodynamic supervision. Nordic Psychology, 61(4), 85-105. doi: 10.1027/1901-2276.61.3.8
Hardy, K. V. (November/December, 1995). Embracing both/and. Family Therapy Networker, 19(6), 42-57.
Hernández, P., Carranza, M., & Almeida, R. (2010). Mental health professionals’ adaptive responses to racial microaggressions: An exploratory study. Professional Psychology: Research and Practice, 41(3), 202-209. doi: 10.1037/a0018445
Hill, C. E. (2014). Helping skills: Facilitating exploration, insight, and action (4th ed.). Washington, DC: American Psychological Association.
Inman, A. G., & DeBoer Kreider, E. D. (2013). Multicultural competence: Psychotherapy practice and supervision. Psychotherapy, 50(3), 346-350. doi: 10.1037/a0032029
Ladany, N., Inman, A. G., Constantine, M. G., & Hofheinz, E. W. (1997). Supervisee multicultural case conceptualization ability and self-reported multicultural competence as functions of supervisee racial identity and supervisor focus. Journal of Counseling Psychology, 44(3), 284-293. doi: 10.1037/0022-0167.44.3.284
Ladany, N., Friedlander, M. L., & Nelson, M. L. (2005). Critical events in psychotherapy supervision: An interpersonal approach. Washington, DC: American Psychological Association.
Lewis, J. A., & Neville, H. A. (2015). Construction and initial validation of the gendered racial microaggressions scale for Black women. Journal of Counseling Psychology, 62(2), 289-302. doi: 10.1037/cou0000062
Miller, S. D., & Duncan, B. L. (2004). The outcome and session rating scales: Administration and scoring manual. Chicago, IL: Institute for the Study of Therapeutic Change.
Murphy-Shigematsu, S. (2010). Microaggressions by supervisors of color. Training and Education in Professional Psychology, 4(1), 16-18. doi: 10.1037/a0017472
Reynolds, A. L. (1997). Using the multicultural change intervention matrix (MCIM) as a multicultural counseling training model. In D. B. Pope-Davis & H. L. K. Coleman (Eds.), Multicultural counseling competencies: Assessment, education, and training, and supervision (pp. 209-226). Thousand Oaks, CA: Sage Publications.
Schön, D. A. (1983). The reflective practitioner: How professionals think in action. New York, NY: Basic Books.
Sue, D. W. (Ed.). (2010). Microaggressions and marginality: Manifestation, dynamics, and impact. Hoboken, NJ: John Wiley & Sons.
Sue, D. W., Capodilupo, C. M., Torino, G. C., Bucceri, J. M., Holder, A. M. B., Nadal, K. L., & Esquilin, M. (2007). Racial microaggressions in everyday life: Implications for clinical practice. American Psychologist, 62(4), 271-286. doi: 10.1037/0003-066X.624.271
Tracey, T. J. G., Bludworth, J., Glidden-Tracey, C. E. (2012a). Are there parallel processes in psychotherapy supervision? An empirical examination. Psychotherapy, 49(3), 330-343. doi: 10.1037/a0026246
Tracey, T. J. G., Bludworth, J., Glidden-Tracey, C. E. (2012b). Parallel process: When does a parallel occurrence carry meaning? Psychotherapy, 49(3), 347-348. doi: 10.1037/a0029115
Watkins, C. E., Jr. (2012). Some thoughts about parallel process and psychotherapy supervision: When is a parallel just a parallel? Psychotherapy, 49(3), 344-346. doi: 10.1037/a0029191
Watts-Jones, T. D. (2010). Location of self: Opening the door to dialogue on intersectionality in the therapy process. Family Process, 49(3), 405-406. doi: 10.1111/j.1545-5300.2010.01330.x
Worthington, R. L., Savoy, H. B., Dillon, F. R., & Vernaglia, E. R. (2002). Heterosexual identity development: A multidimensional model of individual and social identity. The Counseling Psychologist, 30(4), 496-531. doi: 10.1177/00100002030004002
Zetzer, H. A. (2011). White out: Privilege and its problems. In S. K. Anderson & V. A. Middleton (Eds.), Explorations in diversity: Examining privilege and oppression in a multicultural society (2nd ed.) (pp. 11-24). Belmont, CA: Thompson/Wadsworth Publishing.
Zetzer, H. A. (2015). White privilege: The luxury of undivided attention. In B. Bettina & T. Nicholls (Eds.), “I don’t see color”: Personal and critical reflections on white privilege (pp. 119-134). University Park, PA: Pennsylvania State University Press.
Zetzer, H. A., & Reese, R. J. (2014, March). Client feedback in training and supervision: Where the rubber meets the road. Society of Counseling Psychologists Conference, Atlanta, GA.




0 Comments