Psychotherapy Bulletin
Psychotherapy Bulletin

Therapist Dishonesty and Its Association With Levels of Clinical Experience
Authors’ Note: The authors would like to thank Mandy Newman, MA; Mila Kirstie C. Kulsta, BA; Tao Lin, BS; Hannah J. Lindenmeyer, BS; and Amar D. Mandavia, MA, for invaluable assistance in conducting this research.
Clinical impact Statement: This article helps clinicians become aware of the more common forms of therapist misrepresentation that may occur in routine clinical practice. Being aware of these may mitigate therapists’ tendencies to dissemble or make them more conscious of the need to consider the role of therapeutic tact in dialogues with patients.
Introduction
Despite many distinguishing characteristics of the therapeutic relationship, aspects of the dialogue between a therapist and a client can sometimes resemble everyday conversations. Namely, individuals in therapy may occasionally engage in the normative human behavior of lying. Blanchard and Farber (2016) found that 93% of clients report lying or otherwise being dishonest to their therapist in psychotherapy. Client lying behavior largely stems from feelings of shame or embarrassment, making disguising or hiding the truth easier than confronting the truth straightaway. While this is a well-studied phenomenon in psychotherapeutic research, a comparatively under-researched topic is the occurrence of dishonesty on the part of the therapist.
Therapists must use their professional judgment in deciding what is relevant, appropriate, and helpful to disclose or not to disclose to a client in psychotherapy. Traditionally, therapists practicing classic psychoanalysis were instructed to remain objective and anonymous within the therapeutic relationship, precluding the therapist from self-disclosing (McWilliams, 2011). As the practice of psychotherapy has evolved, however, therapist self-disclosure became viewed as a possible tool with which the clinician might normalize a client’s humanness (Audet, 2011; Farber, 2006). Acknowledging fallibility and modeling open expression may strengthen the therapeutic relationship and even encourage client disclosure when used in moderation (Hanson, 2005; Henretty, Currier, Berman, & Levitt, 2014; Ziv-Beiman, 2013). However, not all therapist self-disclosure is equally beneficial. Clients tend to respond more positively to disclosures that reveal information about in-session events rather than disclosures that are overly personal in nature (Audet, 2011).
In an effort to maintain professional boundaries and situate the focus on the client, therapists occasionally choose non-disclosure over self-disclosure. But while non-disclosure is typically clinically appropriate and benign, therapists may also at times engage in concealment, exaggeration, or explicit misrepresentation. Curtis and Hart (2015) were among the first to study patterns of therapist concealment and deception. They found that 96% of therapists reported intentionally keeping information from clients “in order to protect the client,” while 81% reported directly lying to their clients. The topic of therapist lying similarly interests the research team at Columbia University, Teachers College, especially in regard to the frequency and content of therapist lies. The purpose of our current study is to characterize the nature of clinician dishonesty and the demographics of dissembling therapists.
Method
We recruited 271 (N=271) practicing therapists from 38 states and 12 countries to participate in research that investigated the extent to which therapists are occasionally dishonest in psychotherapy. Among this sample, 19.2% were male, 79.7% female, and 1.1% other; 61.7% had been practicing less than 10 years, 21.4% between 10 and 20 years, and 16.9% more than 20 years. When asked about primary therapeutic modality, 11.3% of respondents indicated Dynamic, 21.4% indicated Cognitive Behavioral Therapy/Dialectical Behavior Therapy (CBT/DBT), 1.5% indicated Humanistic, 57.9% indicated Integrative/Eclectic, and 7.9% indicated Other.
The Psychotherapists’ Assessment of Truth, Candor, and Honesty (PATCH) Survey explores the frequency of “therapist lying” across 23 topics:
- Being less than alert
- Forgetting something a client said
- Competence or expertise
- Confidence in being able to help
- Clinical progress
- Clinical availability
- Reasons for canceling/rescheduling
- Reasons for being late/absent
- Conversations with others
- Discussing diagnosis
- Explaining fees
- Discussing training or credentials
- Having outside knowledge
- Own physical/mental health
- Own physical or emotional state
- Aspects of one’s own personal life
- Personal beliefs or values
- Knowledge of someone or something
- Liking/disliking clients
- Feelings of frustration/disappointment
- Romantic/sexual feelings for a client
- Reasons for not taking on a client
- Reason for termination
The frequency of lying for each topic is measured on a 7-point Likert scale with 1 = Never, 4 = Sometimes, and 7 = Frequently. Therapists’ responses to the scaled lying items were averaged to determine the most common topics of lies.
In addition to our lab’s overarching hypothesis that therapists occasionally are less than completely honest more frequently about certain topics, we also hypothesized that more experienced therapists dissemble with greater frequency. Since therapists theoretically become more comfortable navigating conversations in psychotherapy as they gain more experience, we predicted that a longer period of time practicing therapy would correlate to an increased ability to use tools of redirection and tactful concealment. To study this hypothesis, we performed a Latent Class Analysis (LCA) to identify class membership by lying topics. The distinct classes were then compared to the demographic variables “practice years,” “student vs. non-student,” and “age” to determine if experience effects the lying behavior of therapists.
Results
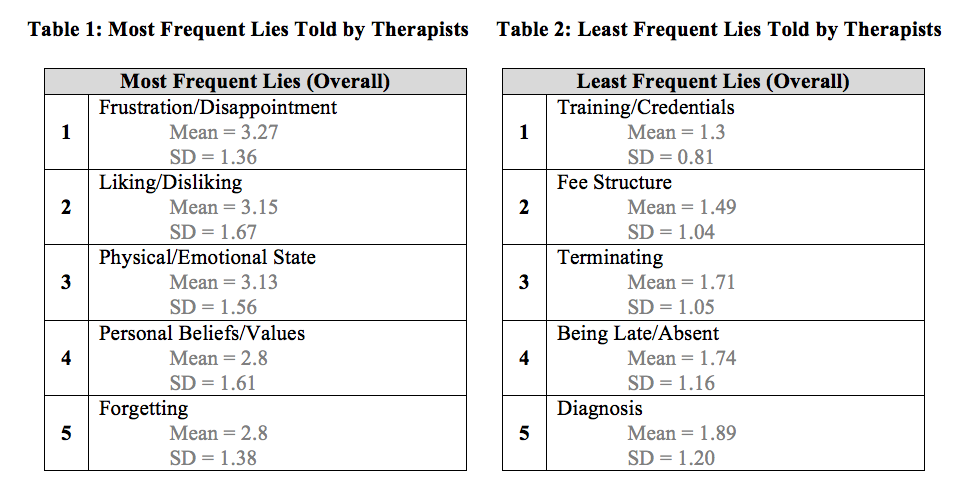
Overall, therapists are most frequently dishonest about their feelings of frustration or disappointment with a client, whether or not they like or dislike a client, their physical or emotional state, their personal beliefs and values, and whether they forgot something a client has said (See Table 1). Conversely, therapists are least frequently dishonest about their training or credentials, their fee structure, reasons for terminating a client, reasons for being late or absent, and a client’s diagnosis (See Table 2).
Even among the topics that are most frequently lied about, different types of therapists dissemble with varying levels of frequency. The LCA distinguished two classes within our data: Class 1 being the therapists who dissemble less frequently and Class 2 being the therapists who dissemble with greater frequency comparatively (2 classes, p = .0008).
Independent t-tests, ANOVAS, and chi-square analyses were run against the demographic variables, revealing significant differences among the demographic characteristics of the classes. Class 1, the less frequently dishonest clinicians, consists of therapists who are currently in a graduate program, are younger than 30 years old, and have less than 5 years in practice. Class 2, the more frequently dishonest clinicians, are the therapists who are already licensed, are older than 30 years old, and have greater than 5 years in practice (see Table 3).

The results of our analyses support the hypothesis that therapists with more experience engage in forms of dishonesty or dissembling with greater frequency than less experienced therapists. Although experience correlates with frequency of dissembling, instances of therapist dishonesty occur relatively infrequently overall. The means of each topic of lie are lower than 4 on our 7-point Likert scale.
Discussion
Compared to graduate students, experienced therapists generally have more freedom and autonomy to construct therapeutic conversations as they see fit. Having completed graduate-level clinical training, experienced therapists have fewer regulatory bodies monitoring their actions. Graduate students, conversely, practice under supervision, which likely regulates the level of student dishonesty. It is far more likely that students would get “caught” in a lie, if not by the client, than by a supervisor. Consequently, it follows that experienced therapists may engage in dishonesty more frequently because they are better able to bend the rules in service of the therapeutic relationship. Still, it bears keeping in mind that the occurrence of any of these deceptions is not especially common.
Although our results indicate that greater experience is correlated with greater rates of dishonesty, it is important to consider the context in which therapeutic untruths are told. The therapeutic relationship requires that the therapist fulfill the role of the primary listener and the client fulfill the role of the primary discloser. Even as the field shifts towards increased levels of therapist self-disclosure, the professional boundaries within the alliance must be maintained. To disclose every thought and feeling a therapist has would reverse the intended roles of therapy, thereby exploiting the position of the client (Audet, 2011). Experienced therapists may be expressly aware of this fact and deliberately choosing to use tactful dishonesty to preserve the roles of the alliance.
The American Psychological Association (APA; 2002) recognizes the necessity and utility of occasional dishonesty, in stating:
In situations in which deception may be ethically justifiable to maximize benefits and minimize harm, psychologists have a serious obligation to consider the need for, the possible consequences of, and their responsibility to correct any resulting mistrust or other harmful effects that arise from the use of such techniques. (p. 3)
Evidently, dishonesty is permissible when used to benefit the client if the consequences of taking such an action are carefully considered. Therapists must acknowledge the potential for resulting mistrust if dishonesty is recognized and left unresolved. Experience may afford therapists the ability to better judge when the benefits of being less than completely honest outweigh the consequences.
As noted above, although instances of dishonesty in psychotherapy are present, our results indicate that they are relatively infrequent and primarily involve the therapist’s feelings towards the client. Both experienced and beginning therapists may recognize that revealing one’s feelings of frustration towards a client or feelings of liking or disliking a client could do more harm than good. Therapists make clinical decisions in consideration of what would benefit the client. Engaging in occasional dishonesty is likely considered in this context as well. In line with this, Curtis and Hart (2015) found that therapists admit to intentionally deceiving clients; however, “mainly with the intent of protecting clients” (p. 290). Therefore, therapist dishonesty may in fact be a necessary tool for the sake of therapeutic tact and protection of the client.
Future Directions
Our findings offer initial insight into the virtually unexplored topic of therapist dishonesty. Therapist lying is clearly an existing and likely consequential phenomenon in psychotherapy that varies by therapists’ demographics. With this knowledge, clinical training in psychotherapy has the potential to expand to include techniques to work with therapeutic lying, including considerations of when lying is clinically justifiable, discussions of how therapists can manage their feelings when they have lied or concealed information, and how therapists might anticipate and deal with the potential clinical consequences of this behavior. To expand on our preliminary findings, our lab plans to conduct follow-up surveys to investigate motivations, justifications, and perceived consequences of therapist dishonesty.
Devlin Jackson, M.A.
Devlin Jackson is a fourth year doctoral candidate with an M.A. in Clinical Psychology from Teachers College, Columbia University, an Ed.M. in Higher Education from Harvard, and a B.A. in Psychology and B.S. in Data Representation from Trinity College.
Cite This Article
Jackson, D., Crumb, C., & Farber, B. (2018). Therapist dishonesty and its association with levels of clinical experience. Psychotherapy Bulletin, 53(4), 24-28.
References
American Psychological Association. (2002). Ethical principles of psychologists and code of conduct. American Psychologist, 57, 1060-1073.
Audet, C. T. (2011). Client perspectives of therapist self-disclosure: Violating boundaries or removing barriers? Counselling Psychology Quarterly, 24(2), 85-100. http://dx.doi.org/10.1080/09515070.2011.589602
Blanchard, M., & Farber, B. A. (2016). Lying in psychotherapy: Why and what clients don’t tell their therapist about therapy and their relationship. Counselling Psychology Quarterly, 29(1), 90-112. http://dx.doi.org/10.1080/09515070.2015.1085365
Curtis, D. A., & Hart, C. L. (2015). Pinocchio’s nose in therapy: Therapists’ beliefs and attitudes toward client deception. International Journal for the Advancement of Counselling, 37(3), 279-292.
Farber, B. A. (2006). Self-Disclosure in Psychotherapy. New York, NY: Guilford Press.
Hanson, J. (2005). Should your lips be zipped? How therapist self‐disclosure and non‐disclosure affects clients. Counselling and Psychotherapy Research, 5(2), 96-104. https://doi.org/
10.1080/17441690500226658
Henretty, J. R., Currier, J. M., Berman, J. S., & Levitt, H. M. (2014). The impact of counselor self-disclosure on clients: A meta-analytic review of experimental and quasi-experimental research. Journal of Counseling Psychology, 61(2), 191-207. http://dx.doi.org/10.1037/a0036189
McWilliams, N. (2011). Psychoanalytic diagnosis: Understanding personality structure in the clinical process. New York, NY: Guilford Press.
Ziv-Beiman, S. (2013). Therapist self-disclosure as an integrative intervention. Journal of Psychotherapy Integration, 23(1), 59-74. http://dx.doi.org/10.1037/a0031783





The analysis was not presented with adequate detail to make for more than a diffuse impression; very little was given in terms of actual analysis and test results in favor of a ‘take my word for it’ approach. Makes for a decent conversation starter, though!
Thank you, it’s great to see this being researched.