Noticing Therapeutic Novelty

Melissa A. Smigelsky, M.A., M.S.
February 19, 2017

Many children participate in the classic science project of nurturing a seedling in a Dixie cup and observing the ensuing course of germination. The child’s primary job is to exercise patience with the process, punctuated by subtle manipulation of the seedling’s environment to ensure ideal growth conditions. Hopefully, in time, the seedling pokes out of the soil in the form of a stem. This is a triumphant moment, and the child often proceeds to tote the small plant around the house, showing off the progress. At this point, a caregiver usually has to step in with a caution that too much jostling may compromise the fragile growth. The child begrudgingly returns the Dixie cup to its designated windowsill, and the waiting and observation continues.
This process parallels therapy, particularly for process-oriented clinicians. The therapist must master the perfect degree of attentiveness, balancing two temptations: overreaction to glimpses of the client’s progress in treatment and under-reaction lulled by the monotonous parts of any therapeutic journey.
How, then, do clinicians notice and nurture novelty, or growth, that is indicative of therapeutic change? Furthermore, how can this novelty be systematically assessed and utilized to promote therapeutic progress?
What Does it Mean to Notice and Nurture Novelty?
Assessing outcomes is an essential part of routine clinical practice. Symptom alleviation, as measured by instruments such as the Beck Anxiety Inventory (Beck & Steer, 1993) or PTSD Checklist for DSM-5 (Weathers et al., 2013), is a commonly utilized metric of therapeutic progress. While amelioration of distress often includes symptom reduction, tracking progress in this way necessitates adherence to an anti-symptom stance. The difficulty with such a perspective is that numerous therapies actually regard symptoms as meaningful and even necessary, and clinical progress can entail adopting an attitude of acceptance, or even gratitude.
Thus while useful in some contexts, symptom reduction measures are not always attuned to novel attitudes that may indicate adaptive progress. Furthermore, symptom measures that focus primarily or exclusively on behavioral changes (including physiological behaviors, such as muscle tension or racing heart) may overlook and therefore miss important changes in cognition that are likely to precede behavior change.
Given the established importance of common factors in therapy and their usefulness in predicting outcomes, assessment of the therapeutic relationship and therapy process provide another type of outcome data. Measures such as the Working Alliance Inventory (Horvath & Greenberg, 1989) and the Session Rating Scale (Duncan et al., 2003) indicate whether the therapeutic bond and collaborative process are functioning well in a given therapeutic relationship during a given session.
Yet, these variables are not problem-specific: a positive working relationship does not necessarily imply therapeutic progress toward addressing client problems (unless perhaps the presenting problem is interpersonal in nature). Furthermore, these measures, and the type of symptom measures noted above, rely on client self-report that may be influenced by social desirability, memory recall difficulty, or other biases.
Clearly there is a need for a means of noticing and nurturing to novelty that does not depend on retrospective reflection, is not beholden to an anti-symptom stance, and yet is also problem-focused.
The Innovative Moments Coding System (IMCS; Gonçalves et al., 2011) is a system for evaluating psychotherapy process research. It is transtheoretical and predicated on the establishment of a problem list derived from the client’s narrative. Rooted in the narrative tradition, the IMCS analyzes the way people tell their stories of themselves, their problems, and their solutions.
Solutions vary and are not pre-determined by the therapist or the type of therapy provided, yet they can be categorized and evaluated according to the type of “unique outcome” they represent. Most importantly, this categorization and analysis can occur moment-by-moment during the therapeutic encounter by a therapist who is tuned into the nuances of the client’s narrative.
What are Innovative Moments?
Innovative moments (IMs) are markers of therapeutic change that contrast with the problematic pattern or narrative: “An IM occurs every time the problematic pattern is challenged and a new way of feeling, thinking, and/or acting emerges that is different from [what] one might expect given the previous functioning” (Gonçalves et al., 2011, p. 497).
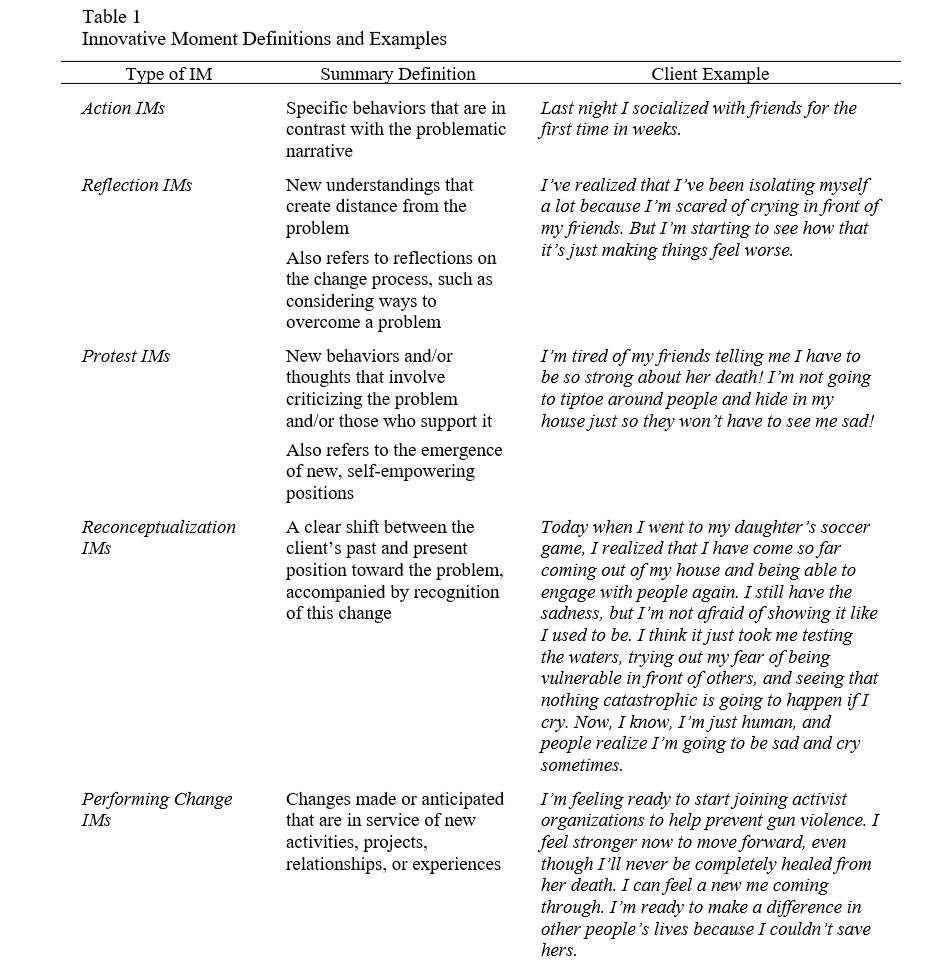
The first step to identifying IMs is to listen carefully to the client’s narrative and derive a problem list, which is an essential step in any case conceptualization. Armed with the problem list, the next step is for the therapist to become familiar with the types of IMs and how they relate to therapeutic outcome. A full discussion of the types of IMs is outside the scope of the present article and is thoroughly covered elsewhere (i.e., Gonçalves et al., 2011).
Brief definitions and client examples from research conducted by our team are provided here (Piazza-Bonin, Neimeyer, Alves, & Smigelsky, 2016; Piazza-Bonin, Neimeyer, Alves, Smigelsky, & Crunk, 2016):
I Recognize an Innovative Moment – How is it Related to Outcome?
The research team in Portugal that developed the IMCS is continually assessing its functionality by exploring both good outcome (GO) and poor outcome (PO) therapy cases (e.g., Cunha et al., 2012; Gonçalves et al., 2012; Mendes et al., 2010; Santos, Gonçalves, & Matos, 2011). This allows for a comparative understanding of the role of IMs, and different types of IMs, in predicting therapeutic outcomes across orientations and presenting problems.
IMs typically occur throughout therapy in both GO and PO cases. However, GO cases have significantly more IMs than PO cases. In GO cases, action, reflection, and protest IMs are present early in therapy and then evolve into reconceptualization and performing change IMs. This evolution is absent or less pronounced in PO cases.
Reconceptualization IMs are central to the formation of a new self-narrative relative to the problem because they provide a meta-perspective that facilitates awareness of how the change occurred.
Performing change IMs generally follow reconceptualization IMs, marking new experiences that arise out of the change. These latter types of IMs are more complex and require a nuanced understanding of the problem, its etiology, and how it is maintained. This is consistent with stage models of change (e.g., precontemplation, contemplation, action, maintenance; McConnaughy, DiClemente, Prochaska, & Velicer, 1989) that suggest progress builds on itself and is facilitated through exploration of both the problem and the unfolding progress.
Therapists should strive to facilitate as many reconceptualization and performing change IMs as possible. According to Gonçalves, Matos, and Santos (2009), therapeutic change results from the elaboration and expansion of IMs. A skillful and attuned therapist may help a client transform a reflection IM to a reconceptualization IM simply by drawing attention to the reflection and helping the client expound upon it. This is more likely to facilitate a good outcome because it moves clients into a deeper understanding of their problems and their solutions.
As a Therapist How Can I Facilitate IMs in Therapy?
The best way to facilitate IMs in therapy is to be a truly integrative therapist, drawing on a variety of modalities to strategically lead from behind as the client moves into deeper self-awareness.
Action IMs are consistent with behavioral interventions that entail doing something concrete in opposition to the problem (e.g., behavioral activation).
Reflection IMs may be best facilitated by cognitive techniques that help a client to think critically and flexibly. Engaging in experiential and emotion-focused interventions, such as chair work (Kellogg, 2007), may bring about protest IMs. These types of interventions are likely already within the toolbox of an integrative therapist. If not, they are relatively easy to adopt with some practice.
How, then, do therapists transform these types of IMs into the more complex types that are most associated with GO cases? This may require moving beyond symptom reduction paradigms and into theories that promote the emergence of a new self-concept, or narrative. Consider this therapeutic exchange between a constructivist therapist and a client, in which the therapist points out a juxtaposition between past and present and encourages further exploration:
T: You are doing something differently with the stress of that grief that is letting the physical manifestation go away. What do you think it is? What makes a useful difference for you there?
C: Maybe it is dealing with it, as opposed to before [when] I kind of did shut down. I did spend a lot of time in my room crying…once I did start back to work and the prospect of going back to school was there, they subsided. I have been finding more creative ways to let it out. (Alves, Mendes, Gonçalves, & Neimeyer, 2012, p. 811).
This exchange focuses on the constructivist goal of helping the client make meaning of her experience. Out of this type of new understanding or sense of meaning, new possibilities can emerge and be enacted as performing change IMs, consistent with a narrative therapy paradigm of re-authoring one’s story. While these examples of modalities are certainly not exhaustive, they hopefully demonstrate the importance of being a truly integrative therapist.
What should I keep in mind when using IMs?
1. IMs are determined by the specific client’s problem list. What is an IM for one client may not be an IM for another client.
2. IMs can be co-constructed. If the therapist senses that a client is on the verge of challenging the problematic narrative, a well-timed and well-constructed reflection, question, or experiential interaction may guide the client into an IM.
3. Therapists can and should help clients stay with and explore IMs when they occur, inviting amplification that can lead to more complex IMs. Never move quickly past an IM!
4. Identifying IMs for clinical, rather than research, purposes allows for more leniency in categorization. However, the therapist should be sure to track complexity of IMs, given the association with good outcomes.
5. Keeping a log of IMs across sessions could be used collaboratively with the client in a later phase of therapy to help consolidate gains, such as by writing a fictional story or creating a work of art that tells the story of the client’s transformation.
Citation
References
Alves, D., Mendes, I., Gonçalves, M. M., & Neimeyer, R. A. (2012). Innovative moments in grief therapy: Reconstructing meaning following perinatal death. Death Studies, 36(9), 795-818. doi:10.1080/07481187.2011.608291
Beck, A. T., & Steer, R. A. (1993). Beck Anxiety Inventory manual. San Antonio, TX: Psychological Corporation.
Cunha, C, Gonçalves, M. M., Hill, C. E., Mendes, I., Ribeiro, A. P., Sousa, I., Angus, L., & Greenberg, L. S. (2012). Therapist interventions and client innovative moments in emotion-focused therapy for depression. Psychotherapy, 49, 536–548.
Duncan, B. L., Miller, S. D., Sparks, J. A., Claud, D. A., Reynolds, L. R., Brown, J., & Johnson, L. D. (2003). The session rating scale: Preliminary psychometric properties of a “working” alliance measure. Journal of Brief Therapy, 3(1), 3-12.
Gonçalves, M. M., Matos, M., & Santos, A. (2009). Narrative therapy and the nature of “innovative moments” in the construction of change. Journal of Constructivist Psychology, 22, 1–23.
Gonçalves, M.M., Mendes, I., Cruz, G., Ribeiro, A., Angus, L., & Greenberg, L. (2012). Innovative moments and change in client-centered therapy. Psychotherapy Research, 22, 389–401.
Gonçalves, M. M., Ribeiro, A. P., Mendes, I., Matos, M., & Santos, A. (2011). Tracking novelties in psychotherapy process research: The innovative moments coding system. Psychotherapy Research, 21(5), 497-509. doi: 10.1080/10503307.2011.560207
Horvath, A. O., & Greenberg, L. S. (1989). Development and validation of the Working Alliance Inventory. Journal of Counseling Psychology, 36, 223–233. http://dx.doi.org/10.1037/0022-0167.36.2.223
Mendes, I., Riberio, A. P., Angus, L., Greenberg, L. S., Sousa, I., & Gonçalves, M. M. (2010). Narrative change in emotion-focused psychotherapy: How is change constructed through the lens of the Innovative Moments Coding System? Psychotherapy Research, 20, 692–701.
Goncalves, M. M., Ribeiro, A. P., Mendes, I., Matos, M., & Santos, A. (2011). Tracking novelties in psychotherapy process research: the innovative moments coding system. Psychother Res, 21(5), 497-509. doi:10.1080/10503307.2011.560207
Kellogg, S. H. (2007). Transformational chairwork: Five ways of using therapeutic dialogues NYSPA Notebook, 19(4), 8-9.
McConnaughy, E. A., DiClemente, C. C., Prochaska, J. O., & Velicer, W. F. (1989). Stages of change in psychotherapy: A follow-up report. Psychotherapy: Theory, Research, Practice, Training, 26(4), 494-503. Retrieved from http://ezproxy.memphis.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=1990-11294-001&site=ehost-live
Piazza-Bonin, E., Neimeyer, R. A., Alves, D., & Smigelsky, M. A. (2016). Innovative Moments in Humanistic Therapy II: Analysis of Change Processes Across the Course of Three Cases of Grief Therapy. Journal of Constructivist Psychology, 1-20. doi:10.1080/10720537.2015.1118713
Piazza-Bonin, E., Neimeyer, R. A., Alves, D., Smigelsky, M. A., & Crunk, E. (2016). Innovative Moments in Humanistic Therapy I: Process and Outcome of Eminent Psychotherapists Working with Bereaved Clients. Journal of Constructivist Psychology, 1-29. doi:10.1080/10720537.2015.1118712
Santos, A., Gonçalves, M. M., & Matos, M. (2011). Innovative moments and poor outcome in narrative therapy. Counselling Psychotherapy and Research, 11, 129–139.
Weathers, F. W., Litz, B. T., Keane, T. M., Palmieri, P. A., Marx, B. P., & Schnurr, P. P. (2013). The PTSD Checklist for DSM-5 (PCL-5). Scale available from the National Center for PTSD at http://www.ptsd.va.gov.
Comments
Be the first to share your thoughts.
Leave a comment
Your email address will not be published. Comments are reviewed before they appear.