Transitioning to Virtual Space



 +1
+1Andrew D. Lokai, M.A. & 4 others
June 1, 2021

In an effort to curb the transmission of the coronavirus disease (COVID-19) that emerged in late 2019, the use of telehealth technology became a necessity for individuals in need of healthcare services to communicate with their healthcare providers (Wosik et al., 2020). Teletherapy, which is a form of telehealth, uses online video conferencing to provide interactive psychological treatment between therapists and patients (Tse et al., 2015). Previous literature has shown that a good working alliance can be virtually established (Norwood et al., 2018). During the COVID-19 lockdown in March 2020, a psychotherapy research program at a major metropolitan medical center in New York City began to offer teletherapy services. Accordingly, a large number of patient-therapist dyads were forced to transition abruptly to this virtual setting. The present study addresses how these dyads adjusted to treatment while facing unprecedented global disruption. This study involved a semi-structured interview and qualitative analysis with the aim of exploring how the transition to teletherapy was experienced by therapists and patients in this program and how this influenced the working alliance.
Method
Participants
The participants in the study included therapists and patients who were participating in the Brief Psychotherapy Research Program affiliated with Mount Sinai Beth Israel (see Muran, 2002; Muran et al., 2018). A total of 10 participants were selected for the study, including five therapists and five patients. Two of the therapists were psychiatry residents, and three were advanced doctoral students in clinical psychology. Their ages ranged between 29 and 32 (M=32.4, SD=1). Four identified as female and one as “other.” Four identified as White, one Latinx. The patients’ ages ranged between 20 and 76 (M=40.4, SD=19.7). Among them, three were male, one female, one identified as nonbinary. Four patients identified as White and one as Latinx.
Procedures and Data Collection
All participants experienced a transition from in-person psychotherapy to teletherapy, having completed at least two in-person sessions before the transition. Only completed cases were selected. Among the 16 identified participants (eight dyads), 10 agreed to participate in the study. Qualitative data were obtained through a semi-structured interview with each of the participants. Each person was interviewed by one of the researchers over the online video conferencing platform Zoom for a duration ranging between 15 minutes and 40 minutes. The interview questions were developed collaboratively by the three researchers, who were all doctoral students in clinical psychology. Each interview began with a standard introduction, an orientation question about the therapy, followed by specific questions targeting the transition to teletherapy and its impact on the working alliance. Follow-up and open-ended questions were used to facilitate the discussion. All the interviews were recorded digitally and transcribed verbatim using the software TranscribeMe. Consent for the interview and recording was sought at the beginning of each interview.
Data Analysis
In this study, Interpretive Phenomenological Analysis (IPA) was used to analyze the data. It was developed by Smith et al. (1995) as a distinctive qualitative approach to explore individuals’ idiographic subjective experiences and is widely accepted by healthcare disciplines, including clinical psychology (Biggerstaff & Thompson, 2008). The transcripts of each participant’s interviews were analyzed by each member of the research team who followed the steps of reading and re-reading the transcripts, noting significant units, identifying emerging themes, and grouping the themes into clusters. Next, consensus meetings were held between the researchers to ensure agreement on the theme clusters. Those that were agreed upon by at least two of the three members were retained on the final list. Lastly, all the theme clusters were further examined and classified in consensus, which resulted in a total of 16 higher-order, superordinate themes. These themes were classified into three groups based on their occurrence: highly common themes (6-9 occurrences), moderately common themes (3-5 occurrences), and unique themes (1 occurrence).
Results
Highly Common Themes
Teletherapy did not affect the working alliance
More participants reported that there was no influence on the alliance in terms of affective bond and agreement on treatment tasks and goals. For example, when asked whether teletherapy has impacted his treatment goals, one patient reported, “I would say really the virtual versus the in-person maybe didn’t really change what we were discussing or what my issues were.” More generally, one therapist stated that “I don’t know that I would say anything about the virtual aspect of our treatment changed the working alliance. I think it’s just the alliance evolved throughout the therapy like it would.”
Teletherapy has potential
There were some therapists who are proponents of teletherapy due to its convenience and flexibility in terms of scheduling that can “dramatically expand[s] access to mental health services.” Additionally, one therapist reported that he virtually shared his process notes with his patient while in session, which was not something he would have done with in-person therapy. This highlighted the benefit of teletherapy as being a useful therapeutic tool which “is actually really cool and probably something [he] should take more advantage of with future clients.” Patients also reported that they were more open to it as it can serve as an alternative for in-person therapy, even though in-person therapy is still preferred. For example, one patient stated, “I would say ultimately it made me much more open to teletherapy, even if I still would prefer an in-person session.”
Negative aspects of teletherapy
Despite some positivity and potential, participants noted negative aspects of teletherapy which include but are not limited to them finding it less effective, difficult to connect emotionally, and an impoverishment of the therapy process. Three therapists reported that they felt teletherapy was less effective, with one stating, “I just felt I wasn’t as effective…I just felt like I couldn’t quite connect with [my patient] in the same way that we did when we were in person.” Another therapist reported that her patient thinks doing “telehealth would be an impoverishment of the process,” while she also felt that it “definitely compromised [the process],” with part of the reason being “it was hard to get to emotional topics” when using this form of treatment.
Teletherapy altered the ritual, process and frame of therapy
Participants noted how teletherapy changed the rituals of going to see a therapist were changed; namely, the physical therapy space was altered, the boundaries loosened, and therapist self-disclosure increased. For example, one patient believed that “there is a certain ceremony to going in-person to the office, getting in that space and having that private space” after he transitioned to teletherapy. Similarly, one therapist compared the difference between “a process for him to get on a train and come to [place] and wait in a waiting room” versus “just clicking, ‘Hello,’ on Zoom or Skype.” Regarding boundaries, one therapist reported that her patient introduced her to people she knew when she was passing her neighborhood one time. Still, one therapist ended up giving her Google Voice number to her patient, which led them to have “a more interactive sort outside of session.”
Teletherapy caused a felt distance between the therapist and patient, which at times was liberating
Interestingly, participants reported that the lack of physical presence in teletherapy made it easier for them to communicate and express themselves without fear of judgment. For example, one patient found that “the less present the other person is, the easier it is to say whatever comes to mind without worrying about whether there’s a reaction or not.” Some therapists also expressed similar views, as one of them pointed out, “there’s kind of that distance there, so it might be a little bit more liberating. He might have let his guard down a little bit.”
Something ineffable is lost with teletherapy
According to some participants, the subtleties of in-person therapy were lost in a virtual setting, although it was difficult for them to articulate what specifics about the visceral presence of the person were missing in teletherapy. One patient stated that “there’s some connection that’s hard to explain from being in the same room as someone when you’re sharing a physical space.” A therapist described teletherapy as “doing that stuff over the screen is just not the same.”
Moderately Common Themes
Switching to teletherapy caused a restarting of the working alliance
Some participants reported feeling a change in the working alliance after transitioning to teletherapy. For example, one therapist stated that she and her patient “definitely had to restart and rebuild” their alliance. This feeling was shared by a patient who found the transition to be difficult because he felt as though he and his therapist were “kind of resetting the relationship a little bit.”
Lack of visual cues with teletherapy
Teletherapy may have compromised participant’s perception of each other. This was reported by two therapists, with one saying that she was unable “to get a good read” on her patient in that she could not observe her patient’s “non-verbal affect and gestures.” Three patients also reported this theme, with one stating that “there’s a lot of cues that she [therapist] was able to spot that maybe aren’t as conveyed as effectively” with teletherapy.
COVID-19 impacted the treatment
This theme illustrated how COVID-19 enhanced the bond between some therapists and their patients as well as affected the goals of treatment. For example, one therapist stated that “the stress of COVID sort of brought us closer.” Another therapist stated that COVID-19 affected her patient’s treatment goal of working on his social and performance anxiety at his workplace because he became “more comfortable communicating virtually rather than in-person” after he had to work at home during the quarantine.
Therapist role shifted during teletherapy
Interestingly, some patients and therapists reported that the role of “therapist” changed during the transition to teletherapy. For example, a therapist stated that he got “into a kind of coaching, problem-solving mindset in a virtual session,” which he would not have gotten into had he been in the same room as the patient. A patient also described that the use of teletherapy resulted in the “normalizing of one’s therapist and making them into more of a person” since they had therapy sessions from their home.
Privacy/safety concerns in doing teletherapy
This theme was reported by two patients, with one stating that he was living with his parents during the quarantine and did not “want them to hear everything that I’m saying,” while the other stated that he was living with his girlfriend and that having therapy at home “doesn’t even feel like a totally safe space to talk.” This theme was supported by a therapist who stated that her patient would at times “get interrupted” by her younger siblings since “she was very much responsible for caring for” them.
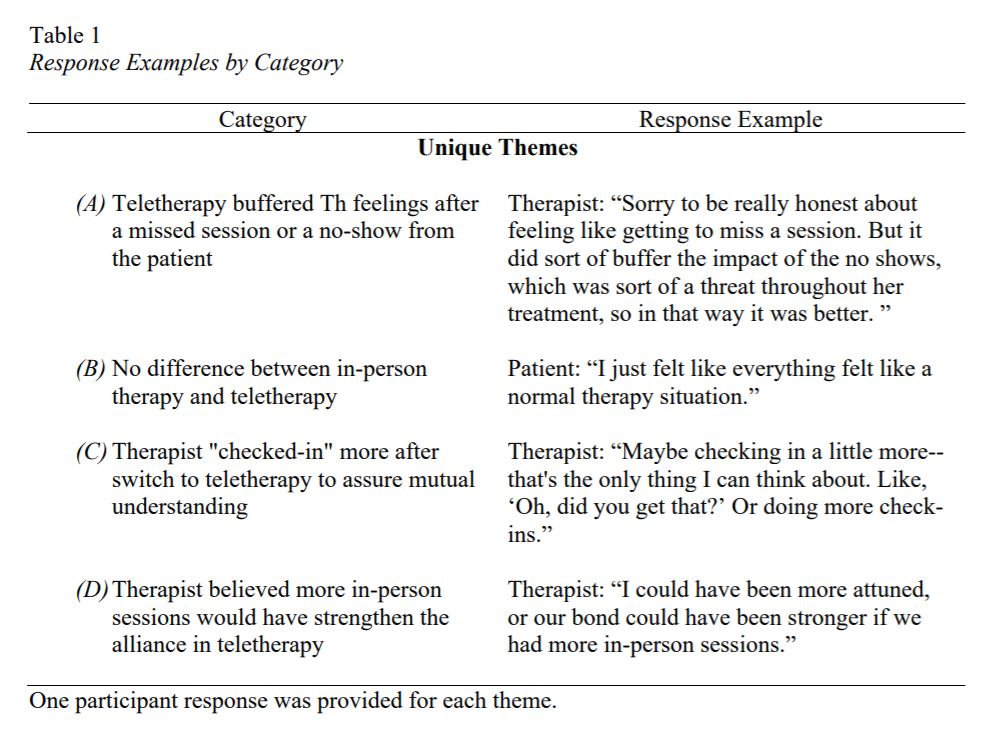
Unique Themes
Unique themes included the following (which are listed here due to space restrictions): Teletherapy buffered therapist feelings after a missed session from the patient; No difference between in-person therapy and teletherapy; Therapist “checked-in” more with the patient after switching to teletherapy to assure mutual understanding; and Therapist believed having more initial in-person sessions would have strengthened the alliance in the alliance in teletherapy (see Table 1 for all the unique themes and supported responses).
Discussion
In considering the working alliance according to Bordin’s (1979) formulation, namely as a combination of shared tasks and goals and the quality of a shared bond, the researchers were able to capture the shift from different angles. Interestingly, when participants were asked outright about changes in the working alliance, nine participants reported that teletherapy did not affect the working alliance (highly common). However, when asked more specifically about the goals, tasks, and bonds, participants reported that COVID-19 affected the goals of treatment (moderately common) that solidarity in COVID-19 enhanced the bond between therapist and patient (moderately common), and that there was an increased focus on tasks as compared with the process of therapy (moderately common). In this way, there is a misalignment between the overall sense of change that was directly reported versus the specific components of the alliance when asked to elaborate.
Another interesting finding was that some therapists became more relaxed in upholding the frame of therapy and maintaining boundaries with their patients. It is possible that since the virtual environment of therapy was taking place in the therapist’s personal space, they felt more relaxed and in a less rigid role than they would have felt if they were doing therapy in a professional setting. This may be related to why one therapist reported feeling less disappointed after a no-show in teletherapy, as she might have felt easier to transition to her own space during that freed-up hour. Another significant finding was that there seemed to be something “ineffable,” or indescribable, about the visceral presence of the other that cannot be reinvented in the virtual setting, which may be the lack of visual cues or the felt distance between therapist and patient.
In thinking about potential limitations to this study, some of the interviews took place months after treatment was completed. Furthermore, the researchers were unable to contact several of the participants, which results in unmatched dyad interviews. The exploratory nature of the present study lends itself to implications of further research. While COVID-19 required that in-person therapy be transitioned to telehealth, it allowed for teletherapy to be considered as a viable alternative option. Now that patients and therapists alike have become somewhat habituated to teletherapy, there is room to expand upon therapist training opportunities to offer therapy virtually.
Tags
Citation
Lokai, A., Chen, L., Terry, K., Eubanks, C., & Muran, J.C. (2021). Transitioning to virtual space: Teletherapy in the time of COVID-19. Psychotherapy Bulletin, 56(2), 29-34.
References
Biggerstaff, D., & Thompson, A. R. (2008). Interpretative phenomenological analysis (IPA): A qualitative methodology of choice in healthcare research. Qualitative research in psychology, 5(3), 214-224. https://doi.org/10.1080/14780880802314304
Bordin, E. S. (1979). The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy: Theory, Research & Practice, 16(3), 252–260. https://doi.org/10.1037/h0085885
Muran, J. C. (2002). A relational approach to understanding change: Plurality and contextualism in a psychotherapy research program. Psychotherapy Research, 12(2), 113–138. https://doi.org/10.1080/713664276
Muran J.C., Safran J.D., Eubanks C.F., & Gorman B.S. (2018). The effect of alliance-focused training on a cognitive-behavioral therapy for personality disorders. Journal of Consulting and Clinical Psychology, 86, 384–397. https://doi.org/10.1037/ccp0000284
Norwood, C., Moghaddam, N. G., Malins, S., & Sabin-Farrell, R. (2018). Working alliance and outcome effectiveness in videoconferencing psychotherapy: A systematic review and noninferiority meta-analysis. Clinical psychology & psychotherapy, 25(6), 797–808. https://doi.org/10.1002/cpp.2315
Smith, J. A., Harré, R., & Van Langenhove, L. (Eds.). (1995). Rethinking methods in psychology. Sage.
Tse, Y. J., McCarty, C. A., Stoep, A. V., & Myers, K. M. (2015). Teletherapy delivery of caregiver behavior training for children with attention-deficit hyperactivity disorder. Telemedicine Journal and E-Health: The Official Journal of the American Telemedicine Association, 21(6), 451–458. https://doi.org/10.1089/tmj.2014.0132
Wosik, J., Fudim, M., Cameron, B., Gellad, Z. F., Cho, A., Phinney, D., Curtis, S., Roman, M., Poon, E. G., Ferranti, J., Katz, J. N., & Tcheng, J. (2020). Telehealth transformation: COVID-19 and the rise of virtual care. Journal of the American Medical Informatics Association: JAMIA, 27(6), 957–962. https://doi.org/10.1093/jamia/ocaa067